The ward round is one of medicine's most information-dense rituals. In 60–90 minutes, a team reviews every patient on the ward, generates a list of actions — blood tests, imaging, medication changes, referrals, discharge planning — and then disperses to execute. The problem: that list lives in someone's head, or scrawled on a paper handover sheet, or split across three different doctors' bleeps.
The Frustration That Started It
As an NHS doctor, I experienced this daily. Tasks would be generated on the ward round and fall through the gaps — not from negligence, but from the structural absence of a shared, prioritised task list that persisted through shift handover. I wanted to build something to fix it.
User Research First
Before writing a line of code, I conducted structured interviews with six doctors — two foundation year doctors, two core medical trainees, and two registrars — to map the actual task management workflow and identify the highest-friction points.
- How do you currently track tasks generated on ward rounds?
- What happens to tasks that aren't completed by the end of your shift?
- What information do you need attached to a task to action it without clarification?
- Where do tasks most commonly fall through the gaps?
What the Research Revealed
Three consistent themes emerged: tasks need to be patient-anchored (not free-floating), urgency and time-sensitivity need to be explicitly visible rather than implied, and handover is the highest-risk moment — the point where task context most often degrades or disappears.
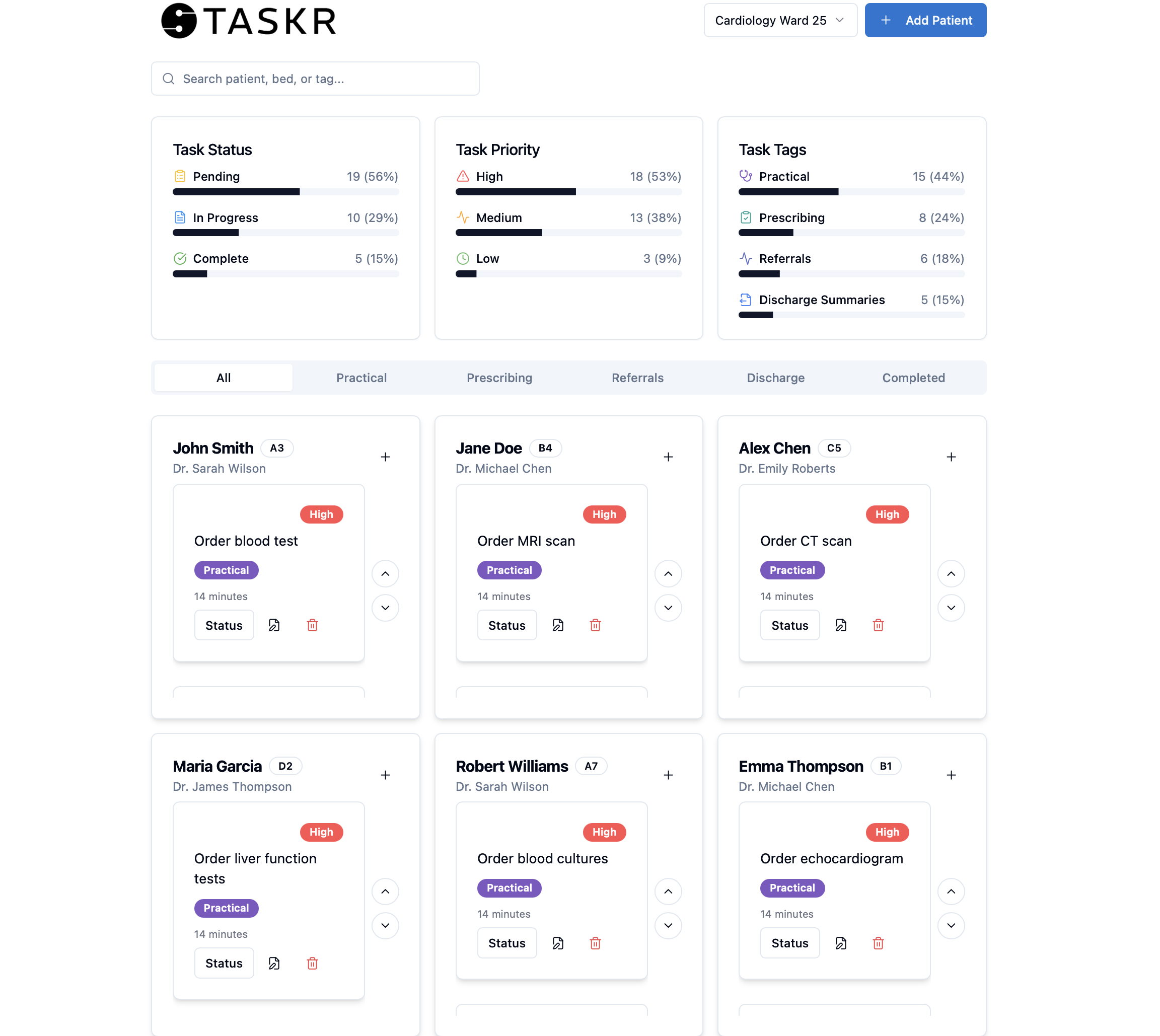
Designing TASKR
TASKR was designed around these insights. The dashboard centres on a patient-anchored task list with three urgency tiers, a structured handover mode that surfaces incomplete tasks with their context intact, and a team view that distributes tasks across the on-call team by workload.
- Patient-anchored task cards with clinical context attached
- Three-tier urgency system: routine, urgent, critical
- Handover mode: generates a structured summary of outstanding tasks with status
- Team distribution: assign tasks to specific doctors, view team workload at a glance
- Audit trail: completed tasks remain visible with timestamp and completing clinician
Validation
After building the prototype, I returned to the same six doctors for usability testing. All six confirmed the core utility of the product. The primary feedback loop led to three iterations: simplifying the task creation flow, adding a 'bleep-free' context field to reduce clarification calls, and building the handover export as a printable format for wards without tablet access.
“TASKR doesn't replace clinical judgement — it just means nothing falls through the gaps because of a broken system.”
— Registrar, user testing session
I documented the full development journey — from initial frustration to validated prototype — in a published article, with the intent of contributing to the growing body of evidence for clinician-led digital health product development.